Original Article - (2019) Volume 7, Issue 3
Comparing the Effect of Guided Visualization and Virtual Reality Techniques on Cannulation Pain in Hemodialysis Patients
Amirreza Nasirzadeh1*, Seyed Farzin Mircheraghi2, Milad Ghodrati1 and Habib Shareinia3
*Correspondence: Amirreza Nasirzadeh, Student Research Committee, Gonabad University of Medical Sciences, Iran, Email:
Abstract
Introduction: The cannulation of arteriovenous fistula [AVF] is a painful procedure in hemodialysis patients. This study aimed to investigate the effect of guided visualization and virtual reality techniques on cannulation pain in hemodialysis patients.
Method: The present pre and post-blinded clinical trial was conducted on 58 hemodialysis patients selected by convenience sampling method. The guided visualization technique was used twice before hemodialysis to attenuate the cannulation pain, followed by the virtual reality technique twice after two weeks. The data collection tools were demographic information form and VAS.
Results: The mean score of pain after intervention was significantly decreased with both techniques and this decrease was more in intervention with virtual reality (p<0.001).
Conclusion: The results showed that both distraction techniques are effective in relieving the severity of cannulation pain in hemodialysis patients, and virtual reality, owing to greater effect, is a proposed intervention to reduce pain in these patients.
Keywords
Guided visualization, Virtual reality, Pain, Cannulation, Hemodialysis
Introduction
Hemodialysis is the most prevalent alternative to renal function [1] and the most commonly used treatment in renal failure patients [2], which promotes the quality of life of hemodialysis patients by prolonging survival and reducing complications. Statistics show that the number of hemodialysis patients will reach 3.5 million in the world by 2020 [1]. There are also over 13,000,000 dialysis patients in Iran, with about 150,000 dialysis sessions each month [3]. According to some studies, the growth rate of this disorder in Iran is about 12% annually [4,5] and 15%, according to others, higher than the global average [3].
Chronic dialysis requires access to safe vessels that can be used for months; therefore, an arteriovenous fistula [AVF] is an appropriate option [1]. About 90% of patients in Iran and about 84% in Europe use AVF for hemodialysis [6]. Despite positive points, AVF has some disadvantages in comparison with other vascular access methods, including the inevitable pain of needle insertion in the fistula [7]. Each dialysis patient undergoes dialysis of approximately 3 times a week and 3 to 4 hours each time, which inevitably tolerates the pain caused by AVF cannulation 3 times a week. This pain will accompany these patients until the end of life unless they perform kidney transplantation [8]. Half of dialysis patients express dissatisfaction with the experience of various types of pain, especially pain caused by AVF cannulation[2]. Reports have shown that 47% of dialysis patients, in addition to fear of cannulation pain, expressed this stage as the most stressful part of dialysis [5]. The main cause of this fear and apprehension is the diameter and length of the needle used for cannulation [7].
The patient pain management is one of the most important nursing cares but there is no certain and standardized method for relieving the cannulation pain [9]. The use of EMLA cream, local anesthesia, local thermotherapy and cryotherapy are interventions that have been previously investigated to reduce the cannulation pain, but the analgesic effect of these interventions has not yet been fully proven[2]. The main problems with the use of local anesthetic drugs are low absorption rate and long exposure time [10], skin rash and allergic reactions in the long term [11]. The adverse effects of chemical drugs [12], the imposition of economic costs [13], and drug tolerance [14] have also led people to relieve pain with complementary medicine. Complementary medicine is an integral part of nursing care [15], which has become popular today, owing to its ease of use, less adverse effect and cost-effectiveness compared to other methods [16]. Based on the available evidence, distraction is one of the most effective nonpharmacologic analgesic methods to reduce the pain associated with aggressive procedures [13,17]. One of the distraction techniques is the guided visualization, which is also part of muscle relaxation [18]. It is a mind-body technique, which can be transmitted through selflearning books and educational videos, or directly through a coach, and used to relieve and manage pain [19]. This technique involves abdominal and diaphragmatic breathing, muscle relaxation and visualization of presence in places such as the seashore, the mountains and the forest, to imagine natural sounds and smells in the mind [19,20]. Related studies have shown that the use of this technique is effective in reducing pain in patients undergoing coronary angiography [19], laparoscopic cholecystectomy [21], and patients with chronic tension type headache [22] and orthopedic surgery [23]. However, some researchers reported the negligible and insignificant influence of guided visualization [20]. In addition, there is little evidence on the effect of guided visualization on reducing the cannulation pain in hemodialysis patients.
The technology plays a key role in today's everyday life. Although the advantages and disadvantages of this technology are still controversial and its use is associated with concerns, it is generally one of the best options for distraction [13]. Previous studies have shown the effectiveness of virtual reality in reducing pain during needle-related procedures [24], pediatric dentistry [25], burn injuries [26,27], venipuncture in children and adults with cancer [28,29], acute and chronic pediatric pain [30] and general pain in adults [31]. Considering that some studies have not shown any difference in the effectiveness of virtual reality to reduce pain, it is still uncertain about the effect of this method to reduce pain [32,33]. Therefore, we examined the hypothesis that virtual reality, compared with guided visualization, could provide a more effective and newer solution for distraction with the aim of reducing the cannulation pain in patients undergoing hemodialysis.
Materials and Methods
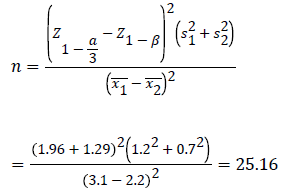
The present pre and post blinded clinical trial was conducted in 2018 after obtaining approval by the Ethics Committee of the Gonabad University of Medical Sciences (GMU.REC.1396.163) and registration code of IRCT20171219037966N3 by the Iranian Registry of Clinical Trials, on eligible hemodialysis patients referred to Imam Reza Hospital of Mashhad and Allameh Behlol Hospital of Gonabad. Sample size was estimated to be about 25 samples per group according to similar study data [34], using the formula of comparing the means for pain variable, and taking 95% confidence interval and 90% test power. Finally, 30 individuals in each group and a total of 60 people were selected, considering the probability of 10% drop-out in samples, (2 of them were excluded due to failure in the first attempt for Cannulation) (Equation 1).
The data were collected after obtaining permission from relevant authorities and receiving informed written consent of the samples selected by the convenience sampling method among all patients undergoing hemodialysis referring to the Imam Reza Hospital of Mashhad and Allameh Behlol Hospital of Gonabad. Before the study, the study objectives were fully explained for patients and they were ensured to leave freely the study at any time. Inclusion criteria were the age range of 18 to 60 years, consciousness of time, place and persons at the time of data collection, minimum reading and writing skills, no history of mental illness, non-diabetic neuropathy, no use of alcohol and drugs, and lack of damaged skin in the intended position. Exclusion criteria were the unwillingness to participate in the study, the failure of venipuncture in the first attempt, and the use of analgesics 24 hours before hemodialysis.
The patients who met the inclusion criterion at first completed a demographic questionnaire including age, sex, educational level, marital status, income level, occupation, and disease-related factors (neuropathy etiology, fistula age, type, site, and duration of dialysis, frequency and duration of dialysis sessions). This part of the questionnaire was prepared after studying the literature on the subject of research, and reviewed and completed using expert opinions. Visual Analogue Scale (VAS) was used to measure the pain intensity. In this method, the patient determined the pain intensity during venipuncture by marking a 10 cm ruler, graded from 0 to 10. The distance between these two points is divided into 1 cm intervals without numbering. The researcher assistant measured and recorded the distance between the zero point and the marked location with a precision of 0.5 cm. In this method, scoring for the pain score is as follows, 0 (no pain), 1-3 (mild pain), 4-6 (moderate pain) and 7-10 (severe pain). This scale is a standard tool whose validity has been confirmed by Ferreira-Valente et al. [35]. Phan et al. verified its reliability by a test-retest method [36].
Study intervention
At the first hemodialysis session, after obtaining informed consent from the patient, the researcher assistant first completed the demographic questionnaire. Then the patient lay on the bed and marked the score of cannulation pain on the VAS. At the second dialysis session, which was the first intervention session, 25 minutes before hemodialysis, the patients were placed in the supine position, with a few deep abdominal and diaphragmatic breaths, closed eyes and comfortable in the best state of relaxation. By providing a completely quiet and relaxed environment, and minimizing environmental stimuli (such as low light room and limited travel), the audio file was displayed to perform mental imagery for 20 minutes, taking into account a sound level between 10 to 21 dB through a device calibrated by an audiologist. In the early minutes of the file, the speaker directs the patients how to prepare for the technique, and then describes the natural environments that they should imagine. When the 15 minutes of the file was played (5 minutes to complete the audio), the fistula was inserted while listening to the audio file, and the pain data was collected by the assistant researcher. After two sessions of intervention by guided visualization, a two-week interval was applied to eliminate the effect of the previous intervention. In the virtual reality group, special glasses were placed on the patient's head 10 minutes before hemodialysis, followed by exhibiting the images designed to reduce pain. After 15 minutes of playing the file and during the watch, the fistula was inserted and then the researcher recorded the pain score. The researcher and data analyst were unaware of the type of intervention performed in the sessions. Given that the patients were hospitalized in two separate hospitals, the same nurse made the cannulation for all patients to minimize the error caused by the difference in the technique of cannulation. In the virtual reality group, the video was displayed through a smartphone (Asus Zenfone 4, 1080 × 1920 pixels, ratio, ~ 401 ppi density) inserted inside the virtual reality headset (VR Box 2, Virtual Reality Headset, Lens diameter: 42 mm, China). To hear the sounds, the headphones were connected to the same smartphone. In the guided visualization group, the same headphones were connected to the smartphone to play audio files.
Statistical analysis
After sampling, the data were analyzed by SPSS version 16 software. First, the Kolmogorov-Smirnov test was used to examine the normality of data distribution. Descriptive statistics were applied to determine the measures of central tendency and dispersion indices for quantitative variables and determine the frequency for qualitative variables. The paired-t test was used to compare the quantitative data of pain variable in the two groups before and after the intervention. The significance level of results from the statistical tests was considered to be less than 5%.
Results
The mean age of the patients was 45.7 ± 0.32 years. The mean duration of dialysis and the mean fistula age was 4.43 ± 0.93 days and 2.84 ± 0.69 years, respectively. Demographic data and disease-related factors are shown in Table 1.
| Variables | Variable levels | Frequency | Percentage (%) |
|---|---|---|---|
| Age (years) | Male | 30 | 51.7 |
| Female | 28 | 48.3 | |
| Educational level | <High school | 22 | 37.9 |
| High school | 17 | 29.3 | |
| Academic | 19 | 32.8 | |
| Occupation | Self-employed | 17 | 29.3 |
| Worker | 17 | 29.3 | |
| Housekeeper | 24 | 41.4 | |
| Smoking | Yes | 6 | 10.3 |
| No | 56 | 89.7 | |
| Fistula site | Right hand | 24 | 41.4 |
| Left hand | 34 | 58.6 | |
| Fistula type | Brachiocephalic | 27 | 46.6 |
| Radiocephalic | 31 | 53.4 | |
| Etiology of nephropathy | Idiopathic | 5 | 8.6 |
| Diabetic | 18 | 31 | |
| Hypertension | 23 | 39.7 | |
| Glomerulonephritis | 5 | 8.6 | |
| Lupus | 1 | 1.7 | |
| Polycystic kidney | 2 | 3.4 | |
| Obstructive or urological problems | 4 | 6.9 |
Table 1: Demographic and disease-related information among the patients
The process of Implementation based on CONSORT flowchart can be seen in Figure 1. Figure 2 shows the cannulation pain score at different time points, and classified results. In the intervention with virtual reality, no patient experienced severe pain. The number of patients with perceived moderate pain was equal in both types of intervention, whereas the number of patients with mild pain in the virtual reality group was greater than the guided visualization in both intervention sessions (Figure 2). The changes in the mean score of pain during intervention sessions can be seen in Figure 3. Both techniques effectively reduced the pain score, and this decrease was more in the virtual reality group. Based on the results of paired t-test, the mean pain scores in the first and second sessions of both techniques were different, and were significantly lower in the second session in the virtual reality group (Table 2 and Figure 3).
| Type of intervention | Pain score (mean ± standard deviation) | Paired t-test | |
|---|---|---|---|
| First session | Second session | ||
| Guided visualization | 4.69 ± 1.17 | 4.10 ± 1.11 | T=9.78 |
| Df=57 | |||
| p<0.001 | |||
| Virtual reality | 4.31 ± 0.98 | 3.86 ± 0.97 | T=7.38 |
| Df=57 | |||
| p<0.001 | |||
| Paired t-test | T=6.13 | T=5.02 | |
| Df=57 | Df=57 | ||
Table 2: Comparison of reductions in mean pain score in the first and second sessions of intervention with guided visualization and virtual reality

Figure 1: Implementation process based on CONSORT flowchart

Figure 2: Number of patients in each hemodialysis session based on the class of pain score

Figure 3: Change in average score during intervention sessions
Discussion
Distraction methods attempt to increase pain tolerance and reduce pain sensation by distracting patient thought [13]. The secretion of endorphins in the brain, following stimulation induced by muscle relaxation techniques, causes a sense of euphoria in patients and relaxation in the muscles, and is effective in relieving pain [37]. The paired t-test result showed that the perceived pain intensity was significantly lower in patients during intervention with virtual reality than in intervention with guided visualization (p<0.001). It is thought that the reason for this issue can be attributed to the existence of a visual effect in interfering with virtual reality. The guided visualization only involves the sound effect, and the patient should use imagination to visualize the environments; that is, if the patient's imagination is not strong, the result will not be desirable. Displaying images with the virtual reality headset makes it easier for patients to work, and thus increase effectiveness. It should be kept in mind that intermittent cannulation leads to the adaptation of some patients with resulting pain, and this may reflect the effect of these techniques less than the actual value [38]. Hua et al. showed that the application of virtual reality when dressing burn patients effectively reduced anxiety and pain, and shortened the time required for treatment [39]. In a study by Brown et al., a distraction method with drug interventions could reduce the pain and anxiety of patients while caring for burn wounds, and could even increase the amount of epithelial tissue reconstruction and repair [40]. A study of people with a sense of discomfort due to chronic pain showed that the use of virtual reality relieved their pain [41]. Tashjian et al. using virtual reality managed to relieve pain significantly in hospitalized patients with a mean score of more than or equal to 3 (out of 10) in the intervention group compared to the control group. According to their claims, the VR can be used as a complementary and safe care option in managing the pain of hospitalized patients [31]. In addition to these studies, several investigations have also focused on the effect of VR on post-stroke rehabilitation [42] and musculoskeletal pain [43]. In our study, the pain intensity during intervention with virtual reality in the first and second sessions of intervention was 22.48% and 30.57% respectively, while the pain relief was 59% in a study by Piskorz et al., aimed at investigating the effect of virtual reality as an intervention to reduce stress and pain induced by venipuncture [38]. Schmitt et al. reported that the intervention with virtual reality reduced the pain up to 27% in the sensory dimension, and up to 32% in the emotional dimension in children with burn injuries [44]. Based on the results of Gershon et al., who evaluated the effectiveness of virtual reality to reduce pain, the venipuncture pain in cancer children was reduced up to 12.7% [45]. This difference may be due to the different nature of the pain types, the various therapeutic procedures, and the type of intervention with the virtual reality (screening or playing games). Moreover, the age difference of the samples could be due to the differences with the present study, because the above studies were conducted on children who are most welcome virtual reality as a new technology. In addition, children have a greater sensitivity to pain and less pain tolerance. In a comprehensive review of the effectiveness of distraction with virtual reality, researchers found that findings from studies on relieving pain induced by venipuncture were inconsistent and did not express the results in line [46].
Comparison of the mean pain score based on the type of intervention showed that the guided visualization had a less pain-lowering effect than the virtual reality. The guided visualization has been effective to reduce pain in patients undergoing surgery [47], elective total knee replacement [48], and generally orthopedic surgery [49]. All of the results of these studies are consistent with the findings of the present study and suggest that the guided visualization can be used as an adjunct to pain management, but further studies with a larger sample size are required to support this conclusion [49,50].
In another study on patients undergoing surgery, the guided visualization could reduce the pain experienced at the second hour after surgery, but had no significant effect on reducing pain in the first hour and the amount of drug used by the patient [51]. The differences in the duration of the intervention, the type of content used and the different therapeutic procedures probably explain this contradiction. In cancer patients undergoing guided visualization, the pain was reported as a dilemma that did not decrease after 30 and 60 days [52].
Nilsson et al. do not recommend using guided visualization as a routine nursing intervention to relieve pain because it has not been beneficial during the vaccination of 11-12-year-old girls. However, further research is required on effective techniques to reduce pain and discomfort associated with invasive and needle procedures [53]. In the study of Chamanzari et al., the guided visualization reduced the total pain score, the duration of pain and the improvement of pain quality in the third day after the operation of patients with fractures, thereby confirming the effectiveness of this method for relieving pain, but did not affect pain intensity [23]. The reason for this difference could be the use of different instruments and various pain experiences in traumatic patients. The guided visualization with relaxing music has not been effective in reducing pain in patients with localized anesthesia under the cutaneous surgical procedures [54].
Conclusion
The virtual reality and the guided visualization, both as distraction techniques, are effective in attenuating the cannulation-induced pain in the hemodialysis patients. However, the virtual reality is a preferred method given the greater relief of pain in this group. Because using virtual reality have a visual effect in comparison with the guided visualization that makes the visualization of the environment easier for the patient and increases the effectiveness of the intervention.
Study Limitations
The pain is a subjective clinical factor that has no apparent presentation and specific clinical sign, except in severe cases. Therefore, we had to make patient scoring for information gathering. There was no possibility of blinding patients according to the nature of the study. As these patients alternatively have intravenous cannulation, their compatibility with this pain increases, which causes the effect of both techniques in this study to be less than actual value.
With regard to the sampling of two hospitals in Iran, the findings of the study will not be able to be generalized to other patients with different characteristics around the world. The lack of evaluation and comparison of the patients' ability to visualize before the study and their different talents in having this ability are among the factors that might lead to errors in the findings of this study.
Conflict of Interest
The authors declare that there is no conflict of interest regarding the publication of this article.
Acknowledgement
This article has been adapted from a research project (code of 1396.163) approved by the Student Research Committee of Gonabad University of Medical Sciences, funded by the Deputy of Research and Technology of the university. The authors would like to thank and appreciate the patients who completed the relevant questionnaires, and all people who collaborated to this project.
References
- Ghoreyshi Z, Amerian M, Amanpour F, et al. Evaluation and comparison of the effects of Xyla-P cream and cold compress on the pain caused by the cannulation of arteriovenous fistula in hemodialysis patients. Saudi J Kidney Dis Transpl 2018; 29:369.
- Mirzaei S, Javadi M, Eftekhari A, et al. Investigation of the effect of EMLA cream, Lidocaine spray, and ice pack on the arteriovenous fistula cannulation pain intensity in hemodialysis patients. Int J Med Res Health Sci 2018; 7:51-7.
- Azimiyan J. Effect of warm footbath on arteriovenous fistula puncture-related pain in dialysis patients. JQUMS 2015; 18:39-45.
- Ekrikpo UE, Udo AI, Ikpeme EE, et al. Haemodialysis in an emerging centre in a developing country: A two year review and predictors of mortality. BMC Nephrol 2011; 12:50.
- Asgari MR, Motlagh NH, Soleimani M, et al. Effect of lidocaine spray on the pain intensity during insertion of vascular needles in hemodialysis patients. Koomesh J Semn Univ Med Sci 2013; 14:271-9.
- Pantelias K, Grapsa E. Vascular access today. World J Nephrol 2012; 1:69-78.
- Çelik G, Özbek O, Yılmaz M, et al. Vapocoolant spray vs. lidocaine/prilocaine cream for reducing the pain of venipuncture in hemodialysis patients: A randomized, placebo-controlled, crossover study. Int J Med Sci 2011; 8:623.
- Hassan A, Darwish MM, El-Samman GA, et al. The impact of cryotherapy on pain intensity at puncture sites of arteriovenous fistula among children undergoing hemodialysis. J Am Sci 2012; 8:1490-500.
- Aliasgharpour M, Mohammadi N, Kazemnejad A, et al. Comparison the effect of lidocaine gel and inhalation of lavender aromatherapy on pain score of arteriovenous fistula puncture in hemodialysis patients. Complementary Med J Faculty Nurs Midwif 2015; 4:1000-11.
- Hijazi R, Taylor D, Richardson J. Effect of topical alkane vapocoolant spray on pain with intravenous cannulation in patients in emergency departments: Randomised double blind placebo controlled trial. BMJ 2009; 338:215.
- Bagheri-Nesami M, Espahbodi F, Nikkhah A, et al. The effects of lavender aromatherapy on pain following needle insertion into a fistula in hemodialysis patients. Complementary Therap Clin Prac 2014; 20:1-4.
- Afshar M, Sattari F, Shadi M, et al. Repairing effects of Iran flora on wound healing. J Birj Univ Med Sci 2015; 22:1-18.
- Gerçeker GÖ, Binay Ş, Bilsin E, et al. Effects of virtual reality and external cold and vibration on pain in 7-to 12-year-old children during phlebotomy: A randomized controlled trial. J Perianesth Nurs 2018; 33:981-9.
- Gallacher J, Elwood P, Pickering J, et al. Benzodiazepine use and risk of dementia: Evidence from the Caerphilly Prospective Study [CaPS]. J Epidemiol Community Health 2012; 869-73.
- Browne NT, Flanigan LM, McComiskey CA, et al. Nursing care of the pediatric surgical patient. 3rd edn. Burlington 2013.
- Wente SJ. Nonpharmacologic pediatric pain management in emergency departments: A systematic review of the literature. J Emerg Nurs 2013; 39:140-50.
- Birnie KA, Noel M, Parker JA, et al. Systematic review and meta-analysis of distraction and hypnosis for needle-related pain and distress in children and adolescents. J Pediatr Psycho 2014; 39:783-808.
- Afshar M, Mohsenzadeh A, Gilasi H, et al. The effects of guided visualization on state and trait anxiety and sleep quality among patients receiving hemodialysis: A randomized controlled trial. Complementary Therap Med 2018; 40:37-41.
- Foji S, Tadayonfar MA, Mohsenpour M, et al. The study of the effect of guided visualization on pain, anxiety and some other hemodynamic factors in patients undergoing coronary angiography. Complementary Therap Clin Prac 2015; 21:119-23.
- Thomas KM, Sethares KA. Is guided visualization effective in reducing pain and anxiety in the postoperative total joint arthroplasty patient? Orthop Nurs 2010; 29:393-9.
- Jong M, Pijl A, De Gast H, et al. The effects of guided visualization on preoperative anxiety and pain management in patients undergoing laparoscopic cholecystectomy in a multi-centre RCT study. BMC Complementary Alterna Med 2012; 12:184.
- Söderberg EI, Carlsson JY, Stener-Victorin E, et al. Subjective well-being in patients with chronic tension-type headache: effect of acupuncture, physical training, and relaxation training. Clin J Pain 2011; 27:448-56.
- Chamanzari H, Raffe S, Modarres GM, et al. Effect of guided visualization on orthopedic operations pain in traumatic patients. Horiz Med Sci 2013; 19:117-22.
- Windich-Biermeier A, Sjoberg I, Dale JC, et al. Effects of distraction on pain, fear, and distress during venous port access and venipuncture in children and adolescents with cancer. J Pediatr Oncol Nurs 2007; 24:8-19.
- Aminabadi NA, Erfanparast L, Sohrabi A, et al. The impact of virtual reality distraction on pain and anxiety during dental treatment in 4-6 year-old children: A randomized controlled clinical trial. J Dent Res Dent Clin Dent Prospects 2012; 117:6.
- Faber AW, Patterson DR, Bremer M. Repeated use of immersive virtual reality therapy to control pain during wound dressing changes in pediatric and adult burn patients. J Burn Care Res 2013; 34:563-8.
- Hoffman HG, Meyer WJ, Ramirez M, et al. Feasibility of articulated arm mounted oculus rift virtual reality goggles for adjunctive pain control during occupational therapy in pediatric burn patients. Cyberpsychol Behav Soc Netw 2014; 17:397-401.
- Chirico A, Lucidi F, De Laurentiis M, et al. Virtual reality in health system: Beyond entertainment. A mini‐review on the efficacy of vr during cancer treatment. J Cellul Physiol 20165; 231:275-87.
- Dascal J, Reid M, Ishak WW, et al. Virtual reality and medical inpatients: A systematic review of randomized, controlled trials. Innov Clin Neurosci 2017; 14:14-21.
- Won AS, Bailey J, Bailenson J, et al. Immersive virtual reality for pediatric pain. Children 2017; 4:52.
- Tashjian VC, Mosadeghi S, Howard AR, et al. Virtual reality for management of pain in hospitalized patients: Results of a controlled trial. JMIR Mental Health 2017; 4:9.
- Gold JI, Kim SH, Kant AJ, et al. Effectiveness of virtual reality for pediatric pain distraction during IV placement. Cyber Psychol Behavior 2006; 9:207-12.
- Nilsson S, Finnström B, Kokinsky E, et al. The use of Virtual Reality for needle-related procedural pain and distress in children and adolescents in a paediatric oncology unit. Europ J Oncol Nurs 2009; 13:102-9.
- Sakhaei S, Motaarefi H, Sadagheyani HE. Comparing the effect of ice massage and acupressure on the intensity of the venipuncture pain in hemodialysis patients. Int J Pharma Bio Sci 2018; 9:164-70.
- Ferreira-Valente MA, Pais-Ribeiro JL, Jensen MP. Validity of four pain intensity rating scales. Pain® 2011; 152:2399-404.
- Phan NQ, Blome C, Fritz F, et al. Assessment of pruritus intensity: Prospective study on validity and reliability of the visual analogue scale, numerical rating scale and verbal rating scale in 471 patients with chronic pruritus. Acta Dermato-Venereologica 2012; 92:502-7.
- Bayoumi M, Al Harbi A, Al Suwaida A, et al. Predictors of quality of life in hemodialysis patients. Saudi J Kidney Dis Transpl 2013; 24:254.
- Piskorz J, Czub M. Effectiveness of a virtual reality intervention to minimize pediatric stress and pain intensity during venipuncture. J Spec Pediatr Nurs 2018; 23 :e12201.
- Hua Y, Qiu R, Yao WY, et al. The effect of virtual reality distraction on pain relief during dressing changes in children with chronic wounds on lower limbs. Pain Manag Nurs 2015; 16:685-91.
- Brown NJ, Kimble RM, Rodger S, et al. Play and heal: Randomized controlled trial of Ditto™ intervention efficacy on improving re-epithelialization in pediatric burns. Burns 2014; 40:204-13.
- Garrett B, Taverner T, McDade P. Virtual reality as an adjunct home therapy in chronic pain management: An exploratory study. JMIR Med Info 2017; 5.
- Henderson A, Korner-Bitensky N, Levin M. Virtual reality in stroke rehabilitation: A systematic review of its effectiveness for upper limb motor recovery. Top Stroke Rehabil 2007; 14:52-61.
- Collado‐Mateo D, Merellano‐Navarro E, Olivares PR, et al. Effect of exergames on musculoskeletal pain: A systematic review and meta‐analysis. Scand J Med Sci Sports 2018; 28:760-71.
- Schmitt YS, Hoffman HG, Blough DK, et al. A randomized, controlled trial of immersive virtual reality analgesia, during physical therapy for pediatric burns. Burns 2011; 37:61-8.
- Gershon J, Zimand E, Pickering M, et al. A pilot and feasibility study of virtual reality as a distraction for children with cancer. J Am Acad Child Adolesc Psychiatry 2004; 43:1243-9.
- Malloy KM, Milling LS. The effectiveness of virtual reality distraction for pain reduction: A systematic review. Clin Psychol Rev 2010; 30:1011-8.
- Singh M, Dalmar A. Use of guided visualization for reduction of pain and anxiety and improved quality of sleep in patients undergoing surgery: A review and meta-analysis. J Patient-Centered Res Rev 2014; 1:146.
- Forward JB, Greuter NE, Crisall SJ, et al. Effect of structured touch and guided visualization for pain and anxiety in elective joint replacement patients-A randomized controlled trial: M-TIJRP. Perm J 2015; 19:18.
- Carpenter JJ, Hines SH, Lan VM. Guided imagery for pain management in postoperative orthopedic patients: An integrative literature review. J Holist Nurs 2017; 35:342-51.
- Meghani N, Tracy MF, Hadidi NN, et al. Part II: The Effects of aromatherapy and guided visualization for the symptom management of anxiety, pain, and insomnia in critically ill patients: An integrative review of current literature. Dimens Crit Care Nurs 2017; 36:334-48.
- Gonzales M, Ledesma C, McAlister C, et al. Effect of guided visualization on postoperative outcomes in patients undergoing same-day surgical procedures: A randomized single blind study. AANA J. 2010; 78:181-8.
- Nooner AK, Dwyer K, DeShea L, et al. Using relaxation and guided visualization to address pain, fatigue, and sleep disturbances: A pilot study. Clin J Oncol Nurs 2016; 20.
- Nilsson S, Forsner M, Finnström B, et al. Relaxation and guided visualization do not reduce stress, pain and unpleasantness for 11‐to 12‐year‐old girls during vaccinations. Acta Paediatr 2015; 104:724-9.
- Alam M, Roongpisuthipong W, Kim NA, et al. Utility of recorded guided visualization and relaxing music in reducing patient pain and anxiety, and surgeon anxiety, during cutaneous surgical procedures: A single-blinded randomized controlled trial. J Am Acad Dermatol 2016; 75:9-585.
Author Info
Amirreza Nasirzadeh1*, Seyed Farzin Mircheraghi2, Milad Ghodrati1 and Habib Shareinia3
1Student Research Committee, Gonabad University of Medical Sciences, Gonabad, Iran2Internal Medicine Department, Medicine Faculty, Gonabad University of Medical Sciences, Gonabad, Iran
3Department of Nursing, Faculty of Nursing and Midwifery, Gonabad University of Medical Sciences, Gonabad, Iran
Citation: Amirreza Nasirzadeh, Seyed Farzin Mircheraghi, Milad Ghodrati, Habib Shareinia, Comparing the Effect of Guided Visualization and Virtual Reality Techniques on Cannulation Pain in Hemodialysis Patients, J Res Med Dent Sci, 2019, 7(3): 55-62.
Received: 28-Mar-2019 Accepted: 05-May-2019